Chapter Twenty: Respiratory Acidosis
Edited by Sophia Ambruso





References
Biff Palmer! Respiratory Acidosis and Respiratory Alkalosis: Core Curriculum 2023
Josh what is sensed- pCO2 or pH and some exploration suggests that it is not settled! Sensing, physiological effects and molecular response to elevated CO2 levels in eukaryotes - PMC and this one with catchy title: Out of thin air: Sensory detection of oxygen and carbon dioxide - PMC
If anna does VOG on Haldane- we’ll need references
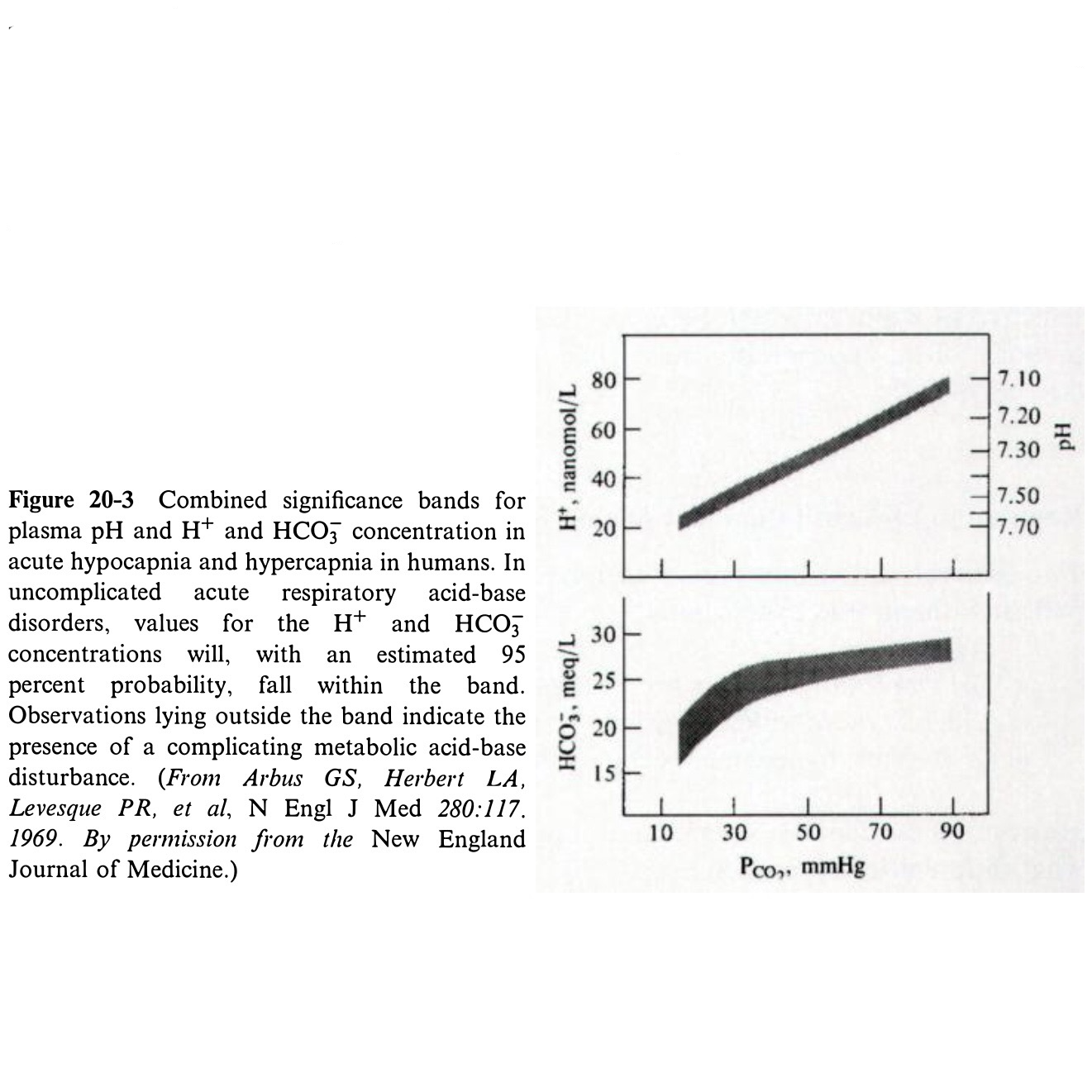
The Response of Extracellular Hydrogen Ion Concentration to Graded Degrees of Chronic Hypercapnia: The Physiologic Limits of the Defense of pH - PMC (this is the correct reference for figure 20-3 reference).
JC shared some info from Dr. Adrogue
Josh mentioned potential differences between people with respect to oxygen sensors and this study of sherpas: [Association of polymorphisms of 1772 (C-->T) and 1790 (G-->A) in HIF1A gene with hypoxia adaptation in high altitude in Sherpas] and this excellent review: Sensing hypoxia: physiology, genetics and epigenetics - PMC
VOG from Amy on renal failure with respiratory acidosis https://pubmed.ncbi.nlm.nih.gov/38936337/
Joel and Roger mention these two perspectives on alkali therapy for respiratory acidosis the first from Adrogué and Madias, the second from David Goldfarb: Alkali Therapy for Respiratory Acidosis: A Medical Controversy - American Journal of Kidney Diseases
Sodium bicarbonate therapy for acute respiratory acidosisJoel mentioned this paper: https://www.nejm.org/doi/pdf/10.1056/NEJM196607212750301 the “carbon dioxide response curve for chronic hypercapnia in man by Bracket, Wingo et al. NEJM 1969
Josh mentioned a study in female ewes that showed a chloride excretion. Acute renal response to rapid onset respiratory acidosis and followed up with this: No renal dysfunction or salt and water retention in acute mountain sickness at 4,559 m among young resting males after passive ascent
This was also studied by Pitts and Giebisch and others: THE EXTRARENAL RESPONSE TO ACUTE ACID-BASE DISTURBANCES OF RESPIRATORY ORIGIN - PMC giebisch and Pitts (the original paper says “with the technical assistance of mary ellen parks and martha MacLeod but on the JCI website, they remedied this and made Parks and MacLeod authors)
Joel mentioned the negative Diablo trial Effect of Acetazolamide vs Placebo on Duration of Invasive Mechanical Ventilation Among Patients With Chronic Obstructive Pulmonary Disease: A Randomized Clinical Trial
Outline: Chapter 20
Respiratory Acidosis
Clinical disorder characterized by
Reduced arterial pH
Elevation of pCO2
Variable increase in HCO3
Increased pCO2 is also seen in metabolic alkalosis
But here it is appropriate
And secondary
PATHOPHYSIOLOGY AND ETIOLOGY
Metabolism generates 15,000 mmol of CO2 per day
CO2 is not an acid, but
Combines with H2O to form H2CO3
H2CO3 dissociates to HCO3 and H+
Most H+ combines with intracellular buffers
Hemoglobin in RBCs
HCO3 leaves the cell via the chloride exchanger
Net result
CO2 generated is primarily carried in blood as HCO3
Little change in pH
Process reverses in the alveoli
As H+Hb is oxygenated, H+ is released
H+ combines with HCO3 to form H2CO3
Carbonic anhydrase breaks H2CO3 into H2O and CO2
CO2 is exhaled
Control of Ventilation
Alveolar ventilation
Provides oxygen for oxidative metabolism
Eliminates metabolically produced CO2
Main stimuli for respiration
Reduced arterial pO2
Increased pCO2
Controlled in chemosensitive areas of the medulla
Respond to CO2-induced changes in cerebral pH
Initial hypoxic stimulation comes from carotid body chemoreceptors
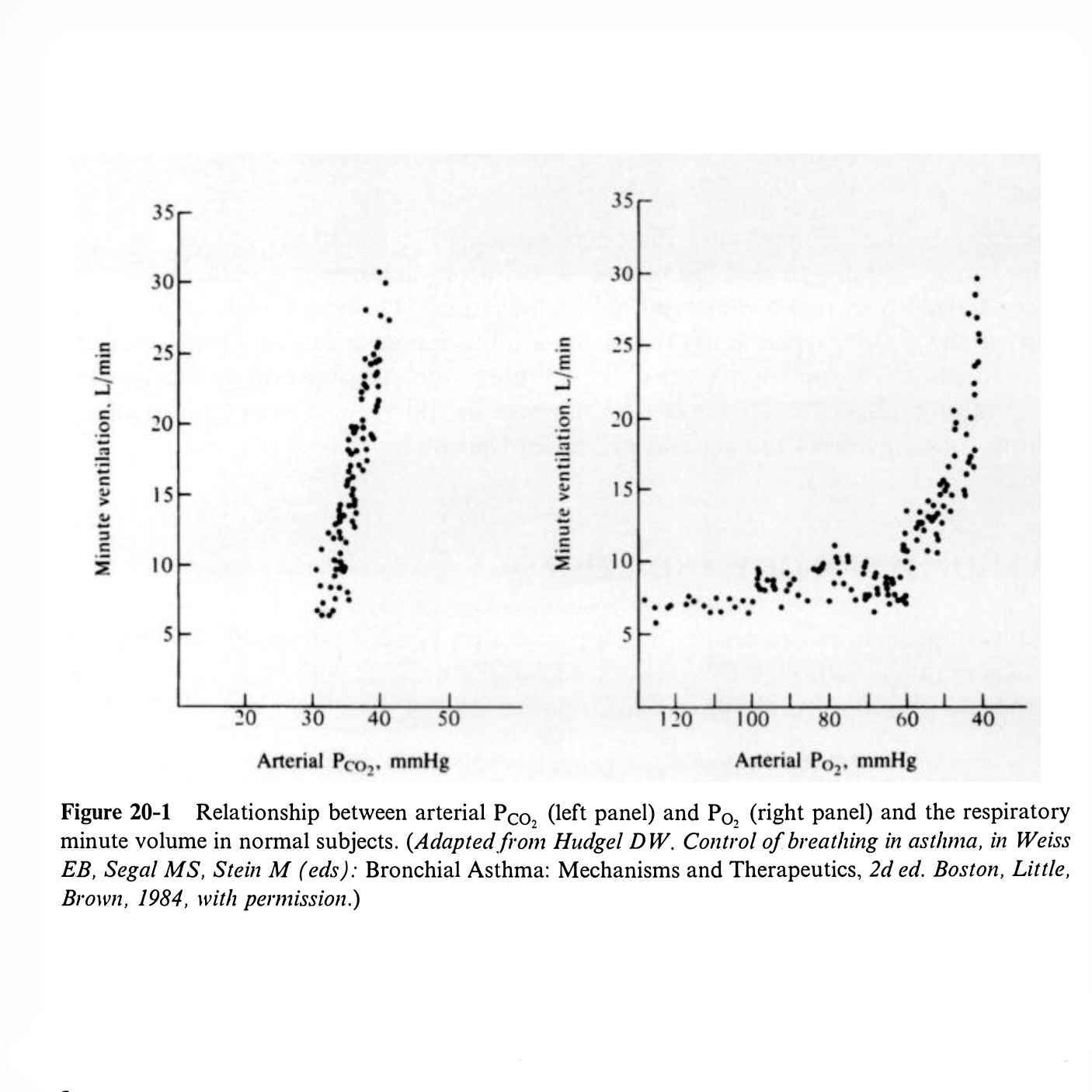
Figure 20-1 is wild
pCO2 is maintained within narrow limits despite
Large daily CO2 load
Variable respiratory quotient
Variable metabolic rate
Minute ventilation rises 1–4 liters for every 1 mmHg rise in pCO2
pO2 does not significantly stimulate ventilation until arterial pO2 <50–60 mmHg
Actually starts earlier
Increased ventilation lowers pCO2 which inhibits respiration
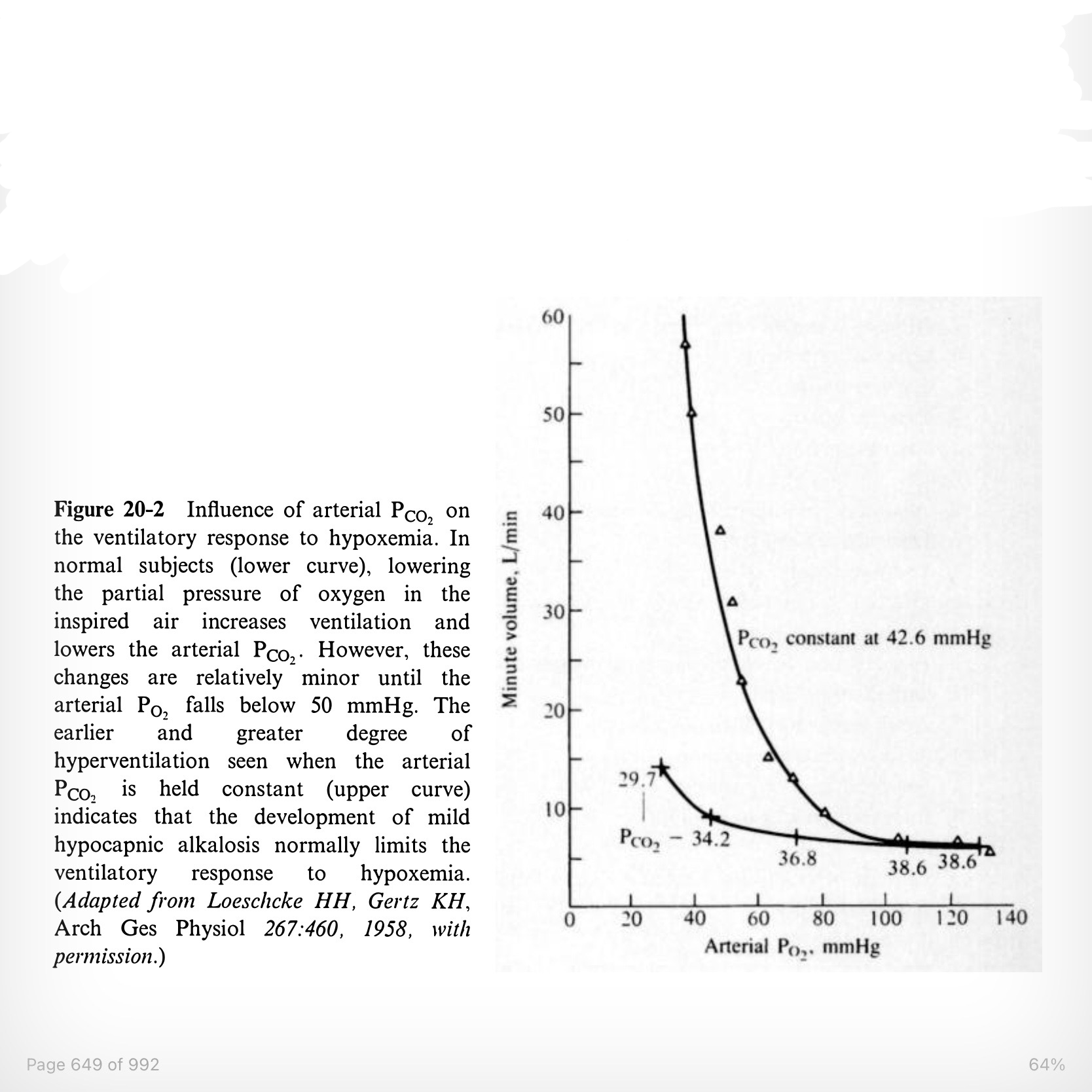
If pCO2 is fixed, pO2 of 70–80 mmHg will stimulate respiration
Figure 20-2
Development of Hypercapnia
Because CO2 is such a potent respiratory stimulant
Respiratory acidosis is usually due to decreased minute ventilation
Not increased CO2 production
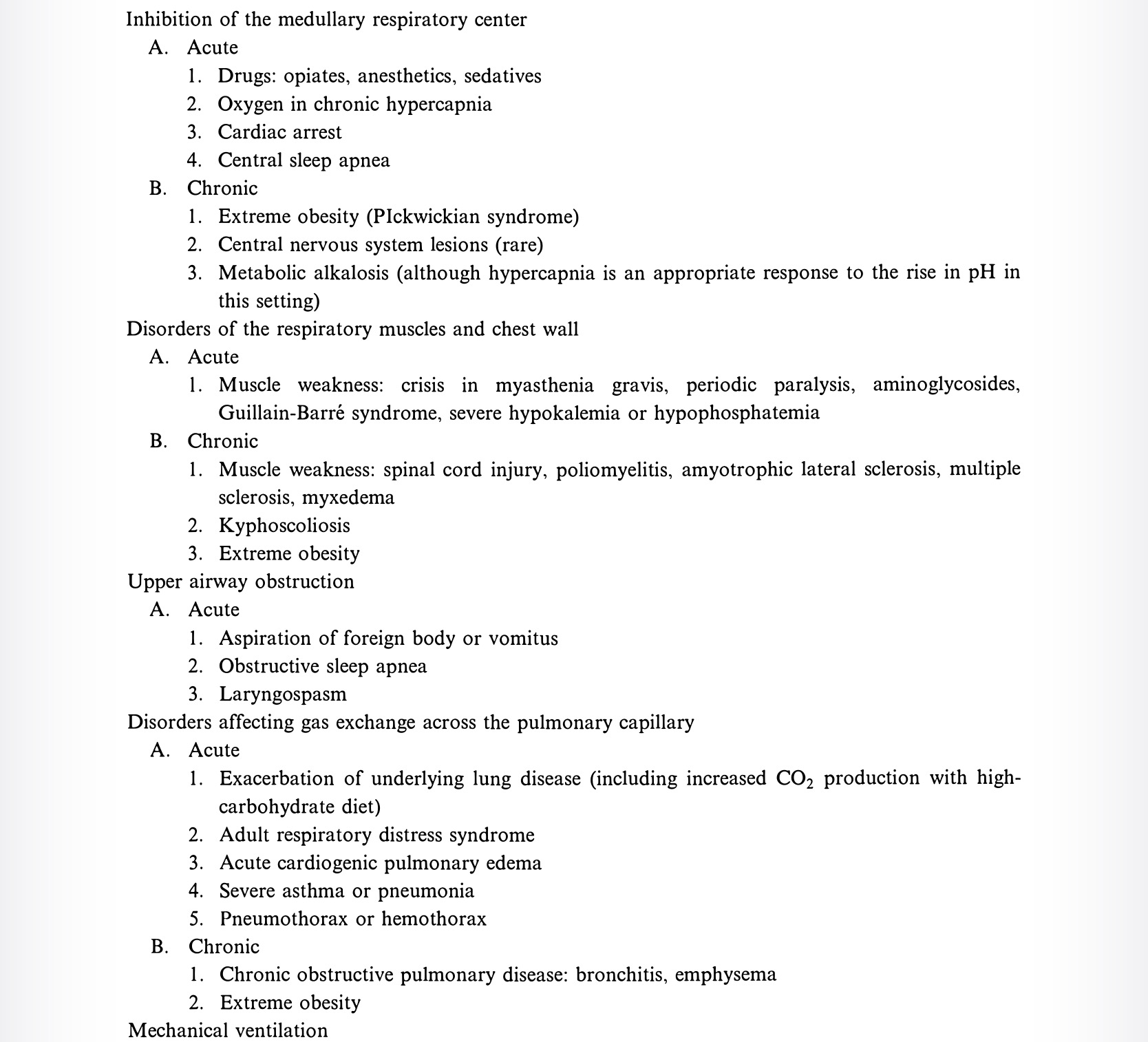
Table 20-1 lists causes
CO2 retention in intrinsic pulmonary disease
Due to ventilation/perfusion mismatch
Hypercapnia is beneficial
Allows excretion of produced CO2 at lower minute ventilation
Consequences
Increased pCO2 decreases pH
Increased bone and cellular buffering
Increased renal H secretion
Raises serum HCO3
Relationship Between Hypercapnia and Hypoxemia
All hypercapnic patients breathing room air have lower alveolar and arterial pO2
Total alveolar partial pressures must equal atmospheric pressure
Hypoxemia generally occurs earlier and is more severe than hypercapnia
CO2 diffuses 20× faster than O2
Compensation by increasing ventilation in normal lung segments
Improves CO2 elimination
Cannot substantially increase O2 because Hb already saturated
Acute asthma example
Mucus plugging and bronchoconstriction cause hypoxemia
Hypoxemia and mechanoreceptors stimulate ventilation
Produces respiratory alkalosis
Respiratory acidosis is a late finding
Respiratory resistance rises
Maximal minute ventilation falls
pCO2 rises
First normalizes
Then becomes elevated
Therefore
Normal pCO2 in acute asthma indicates severe disease
Generalization to other lung diseases
Even small increases in pCO2 indicate severe respiratory disease
Hypoxemia-induced hyperventilation delays hypercapnia
But there is 16-fold variability in sensitivity to hypoxemia
Less sensitive individuals develop respiratory acidosis more readily
Regulation of Ventilation in Chronic Respiratory Acidosis
Two common statements
Respiratory centers become less sensitive to CO2 over time
Hypoxia becomes the primary respiratory stimulus
Insensitivity to CO2
Chemoreceptors primarily respond to pH
Chronic respiratory acidosis increases HCO3
Therefore less pH change despite elevated pCO2
Less respiratory stimulation
Worsening hypercapnia and hypoxia
Similarly
Diuretic-induced metabolic alkalosis suppresses ventilation
Dependence on hypoxemia
Patients with chronic respiratory acidosis rely on hypoxia to drive breathing
Loss of CO2 stimulation due to
Renal compensation raising HCO3
Diuretics raising HCO3
Making pH less dependent on pCO2
Hypoxia drives ventilation when pO2 falls below ~80
Makes oxygen administration potentially dangerous
Can suppress respiratory drive
Oxygen also reverses hypoxic vasoconstriction
Increases V/Q mismatch
Acute Respiratory Acidosis
Body poorly adapted to acute elevations in pCO2
HCO3 cannot buffer H2CO3
See Eq 20-4
Must use hemoglobin and proteins as buffers
See Eq 20-5
HCO3 rises 1 mEq/L for every 10 mmHg increase in pCO2
Example
pCO2 rises to 80
HCO3 rises to 28
pH falls to 7.17
Without buffering
pH would be 7.10
Not dramatically different
Etiology
Acute exacerbations of lung disease
Severe asthma
Pulmonary edema
Drug overdose
Sleep apnea syndromes
Central
Obstructive
Mixed
Chronic hypercapnia uncommon in isolated OSA
CO2 cleared during wakefulness
OSA + structural lung disease + obesity
Reduced daily alveolar ventilation
Persistent CO2 retention
Obesity hypoventilation syndrome
Mechanical ventilation
Inadequate respiratory rate can cause respiratory acidosis
Fixed ventilation means increased CO2 production can cause respiratory acidosis
Cardiac arrest
Suggests sodium bicarbonate
Arterial ABG may miss severity due to poor pulmonary blood flow
Mixed venous blood may be better guide
Enteral or parenteral overfeeding
Chronic Respiratory Acidosis
After 3–5 days
HCO3 rises 3.5 mEq/L for every 10 mmHg rise in pCO2
Example
pCO2 = 80
4 × 3.5 = 14
HCO3 should be 38
pH ~7.30
Allows tolerance of pCO2 values of 90–110
Exogenous alkali
Unnecessary
Useless
Easily excreted
Etiology
COPD
Genetic variation in sensitivity to hypoxemia and CO2
Blue bloaters
Low response to CO2
Hypoxia becomes primary respiratory stimulus
Pink puffers
Strong CO2 response
Tachypnea develops early
Compensation for loss of lung tissue
Pickwickian syndrome
Obesity hypoventilation syndrome
Book mistakenly says hyperventilation
Chest wall weight impairs breathing
More complex than that
Weight loss only helps some patients
Progesterone can improve condition
Suggests central respiratory defect
May coexist with OSA
Unlike OSA, Pickwickian patients have chronic respiratory acidosis
SYMPTOMS
Neurologic
Headache
Blurred vision
Restlessness
Anxiety
Can progress to
Somnolence (CO2 narcosis)
Tremor
Asterixis
Delirium
Increased CSF pressure
Papilledema
Due to increased cerebral blood flow
Symptoms due to CSF acidemia
Less common in metabolic acidosis
HCO3 crosses BBB poorly
Less common in chronic respiratory acidosis
Less severe acidemia
Arrhythmias
Peripheral vasodilation
Hypotension
Particularly when pH <7.1
Cor pulmonale
Peripheral edema
Can occur despite normal GFR
Suggests relationship between respiratory acidosis and renal sodium handling
Or possibly hypoxia
DIAGNOSIS
Last full paragraph on page 659 discusses ambiguity of ABGs
Nicely done
Figure 20-6
Two additional examples
Both instructive
Final sentence
“In summary, the confidence bands are useful guides in the interpretation of acid-base measurements. However, this interpretation cannot proceed in a vacuum and must be correlated with a complete history and physical examination.”
Use of the Alveolar-Arterial Oxygen Gradient
Derivation
1 atmosphere = 760 mmHg
Water vapor = 47 mmHg
Nitrogen = 563 mmHg
Leaves ~150 mmHg oxygen
No net movement of water or nitrogen
Therefore O2 + CO2 must account for remaining pressure
PAO2 = PIO2 − PACO2
Must multiply CO2 by 1.25 to account for respiratory quotient
PAO2 = PIO2 − (1.25 × PACO2)
Since CO2 diffuses rapidly
PACO2 ≈ PaCO2
Normal values
PIO2 = 150
PaCO2 = 40
PAO2 = 150 − (1.25 × 40)
PAO2 = 100
Normal A-a gradient
5–10 mmHg in young adults
15–20 mmHg in elderly
A-a gradient = PAO2 − PaO2
Combined equation
A-a gradient = PIO2 − (1.25 × PaCO2) − PaO2
A-a gradient increased in intrinsic pulmonary disease
Oxygen has difficulty entering blood
May also be increased in some extrapulmonary disorders
No explanation given
Normal A-a gradient argues against pulmonary disease
Suggests
Central hypoventilation
Primary metabolic alkalosis
Chest wall weakness
Respiratory muscle weakness
TREATMENT
Complete discussion beyond scope of text
Acute Respiratory Acidosis
Give oxygen for hypoxia
Correct underlying cause of hypercapnia
Or intubate
Sodium bicarbonate
Role not well defined
May help if pH <7.15
Especially severe asthmatics on ventilators
Avoid in
Pulmonary edema
Can worsen congestion
CNS effects
Does not protect CNS because HCO3 does not cross BBB
Increased pCO2
Must monitor mixed venous pH
Late metabolic alkalosis
Rare according to author
Tromethamine (THAM)
Binds hydrogen
Rapidly cleared by kidneys
“THAM is of uncertain safety”
Chronic Respiratory Acidosis
Goals
Adequate oxygenation
Improve effective alveolar ventilation if possible
Rarely need to treat pH directly
Beware oxygen
Can act as respiratory depressant
Dietary modifications
Reduce carbohydrates
Improves respiratory drive for unclear reasons
Weight reduction
Improves respiratory mechanics
Target pO2 60–65
Reduces pulmonary vasoconstriction
Reduces secondary polycythemia
Mechanical ventilation
Lower pCO2 gradually
Rapid correction can induce metabolic alkalosis
Seizures
Coma
Effect of superimposed metabolic alkalosis
Metabolic alkalosis depresses ventilation
Discontinue diuretics
Give saline
Acetazolamide
Acetazolamide caveats
Need appropriate bicarbonate target, not normal
Can transiently increase pCO2 before diuretic effect
May be due to partial inhibition of carbonic anhydrase in RBCs needed for CO2 carrying capacity