Chapter Twenty One: Respiratory Alkalosis
Edited by Nayan Arora
References
Chapter 19, Part 3 August 30, 2023Biff Palmer’s Ted Talk-Why not? Biff Palmer at TEDxSMU 2013
Anna mentioned this issue of lactic acidosis in a panic disorder: The Lactic Acid Response to Alkalosis in Panic Disorder | The Journal of Neuropsychiatry and Clinical Neurosciences
Reminder of important clinical lesson: Lactate: panicking doctor or panicking patient? - PMC
Melanie regaled the group with an excerpt (page 351) Cohen, J. J., Kassirer, J. P. (1982). Acid-base. United States: Little, Brown.
Biff Palmer! Respiratory Acidosis and Respiratory Alkalosis: Core Curriculum 2023
Melanie loves this study of chronic respiratory alkalosis on participants to traveled to the High ALpine research station on the Jungfraujoch in the Swiss Alps Chronic Respiratory Alkalosis — The Effect of Sustained Hyperventilation on Renal Regulation of Acid–Base Equilibrium | NEJM (and here’s a great picture: Services: Jungfraujoch Research Station - Climate and Environmental Physics (CEP)
JC mentioned that there are cells in the carotid body which are called glomus cells Neurobiology of the carotid body.
JC discussed respiratory alkalosis in cirrhosis and here’s a review he had melanie write that addresses this topic: Acid Base Disorders in Cirrhosis - Advances in Kidney Disease and Health and here are some reviews he likes: The hyperventilation of cirrhosis: progesterone and estradiol effects and Acid-base disturbance in patients with cirrhosis: relation to hemodynamic dysfunction and Blood-Brain Barrier Permeability Is Exacerbated in Experimental Model of Hepatic Encephalopathy via MMP-9 Activation and Downregulation of Tight Junction Proteins
The finding of respiratory alkalosis in pregnancy is not a new concept. Here’s a study from 1962: Acid-base balance of arterial blood during pregnancy, at delivery, and in the puerperium - American Journal of Obstetrics & Gynecology
Melanie reminded us of the Charlie Brown sad face that occurs after bicarbonate infusion and delay in bicarbonate movement to the CSF! Spinal-Fluid pH and Neurologic Symptoms in Systemic Acidosis | NEJM (part 2 of chapter 11)
Josh mentioned this report from Andrew Tarulli (a great neurologist previously at BIDMC who has moved to Overlook Hospital in NJ) Central Neurogenic Hyperventilation: A Case Report and Discussion of Pathophysiology | Allergy and Clinical Immunology | JAMA Neurology
He also mentioned this important transporters that affect the pH. The choroid plexus sodium-bicarbonate cotransporter NBCe2 regulates mouse cerebrospinal fluid pH
Refractory Central Neurogenic Hyperventilation: A Novel Approach Utilizing Mechanical Dead Space
Outline: Chapter 21
Respiratory Alkalosis
Increased pH, low pCO2, variable reduction in HCO3
Differentiate from metabolic acidosis where pH is decreased
(but pCO2 and HCO3 are likewise decreased)
PATHOPHYSIOLOGY
Primary decrease in pCO2 when effective alveolar ventilation is increased beyond that needed to eliminate daily CO2 production
How does the body respond to hypocapnia
Mass action
Reduction in H+ induced by hypocapnia can be minimized by lowering HCO3
One: rapid cell buffering
Two: later decrease in net renal acid secretion → lower HCO3
These two strategies explain the difference between acute and chronic respiratory alkalosis
Acute Respiratory Alkalosis
Within 10 minutes, H ions move into extracellular fluid
H+ combines with HCO3 → fall in plasma HCO3
Converted to CO2 and H2O
H+ comes from intracellular buffers
Protein, phosphate, hemoglobin
H+ may also come from alkalemia-induced increase in cellular lactic acid production (1)⁉️
Enough H+ enters ECF to lower HCO3 by 2 mEq for each 10 mmHg decrease in pCO2 (Fig 20-3)
Example: pCO2 falls to 20
HCO3 falls by 4 → ~20 mEq/L
pH ~7.63
Not very efficient at protecting pH
Without compensation pH would be ~7.70
Chronic Respiratory Alkalosis
Compensatory ↓ renal H secretion
Begins within 2 hours
Not complete for 2–3 days
Due to parallel rise in tubular cell pH
Manifested by
HCO3 loss
Decreased NH4 in urine
4 mEq drop in HCO3 for each 10 mmHg decrease in pCO2
Example: pCO2 20 → HCO3 16 → pH ~7.53
ETIOLOGY
Respiration governed by two sets of chemoreceptors
Central (respiratory center in brainstem)
Peripheral (carotid bodies at bifurcation, aortic bodies at arch)
Central chemoreceptors
Stimulated by ↑ pCO2 or metabolic acidosis
Peripheral chemoreceptors
Stimulated by hypoxia (and acidosis)
Thus hyperventilation can be produced by
Hypoxemia
Anemia
Reduction in arterial pH
Other stimuli
Pain
Anxiety
Mechanoreceptors
Direct stimulation of respiratory center
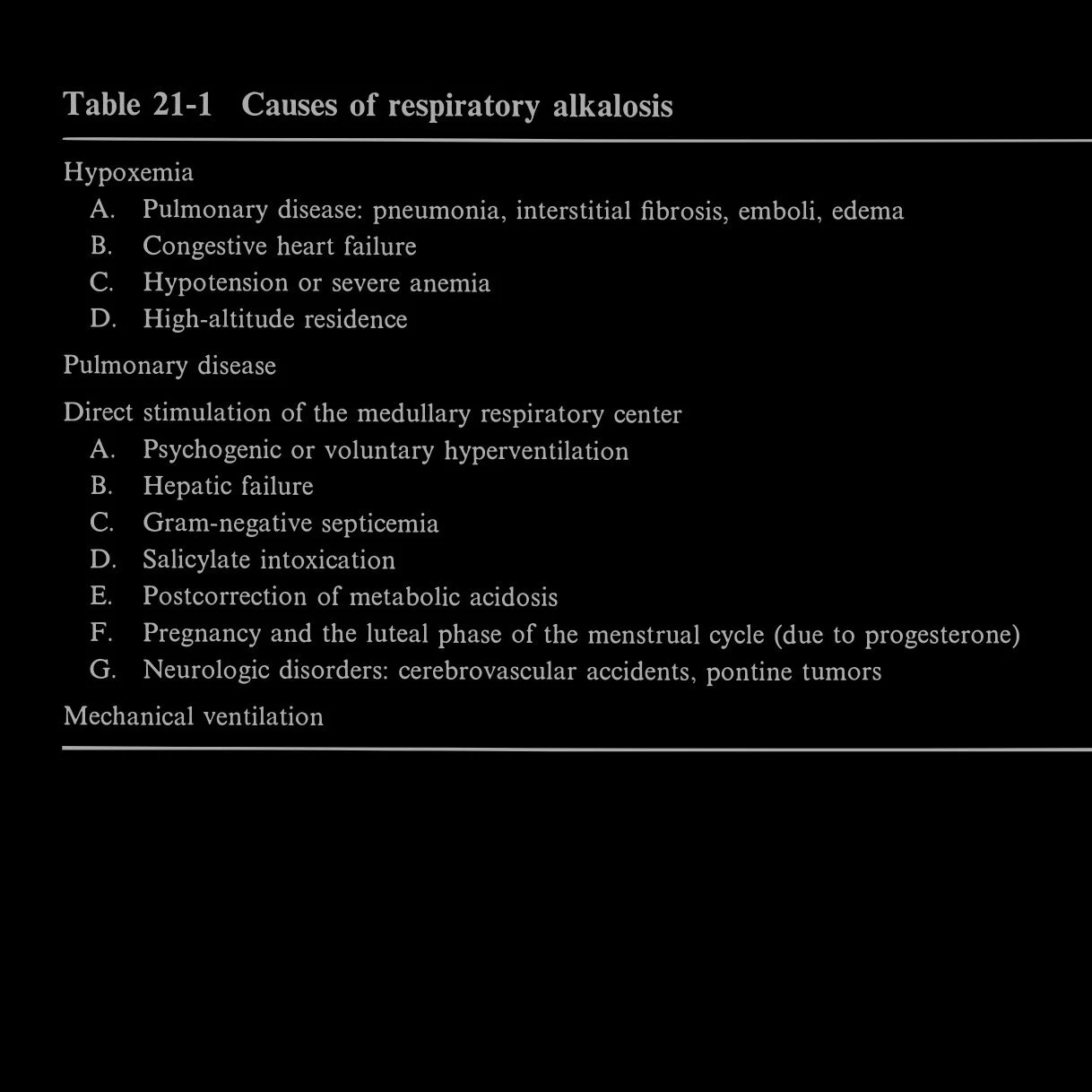
Table 21-1
Hypoxemia
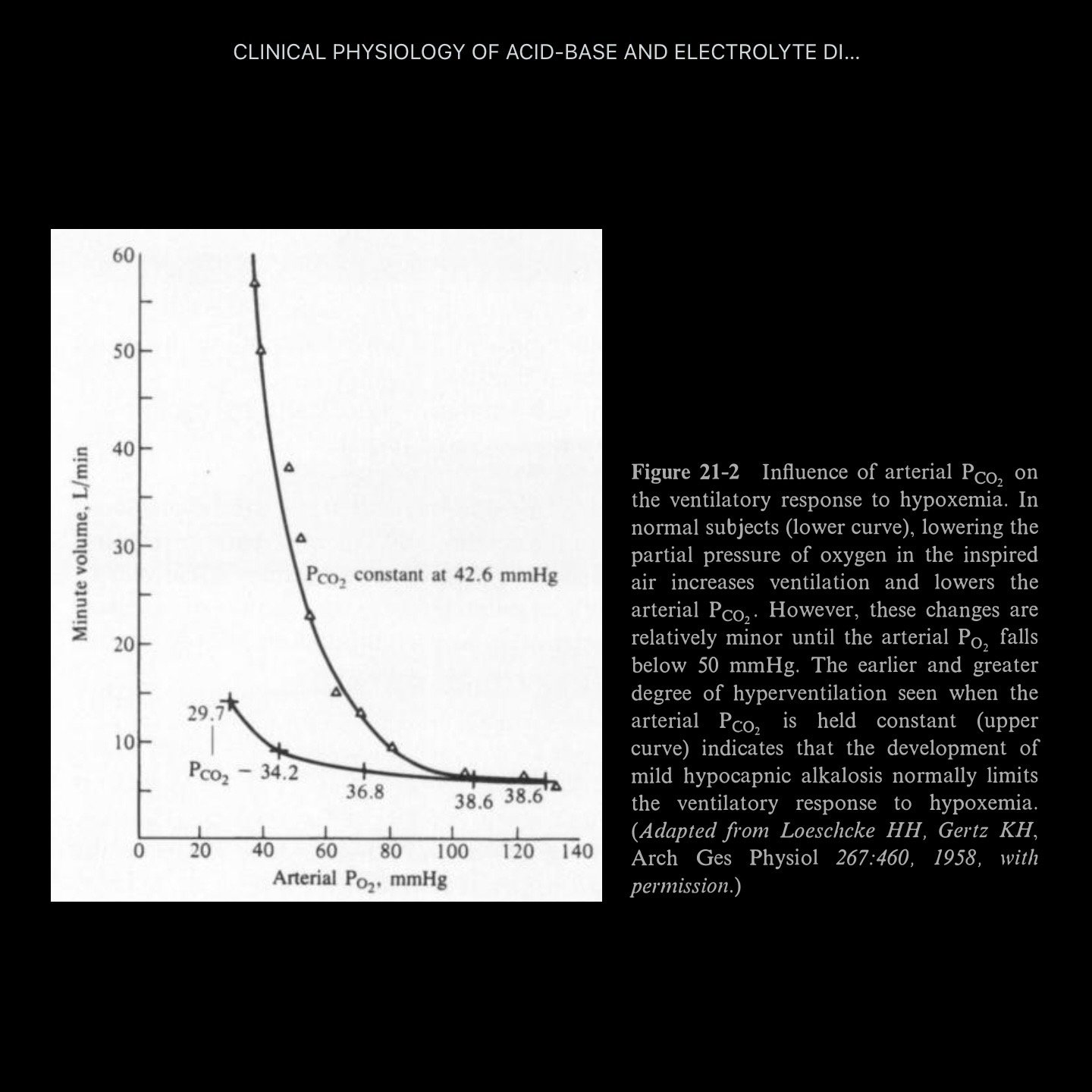
Respiratory response occurs in stages
Stage 1
Peripheral chemoreceptor activation
Hyperventilation → respiratory alkalosis
Increased cerebral pH inhibits central respiratory center
Limits hyperventilation
No significant hyperventilation until pO2 < 50–60 mmHg
If lung disease prevents pCO2 reduction
Hypoxia stimulates ventilation at PaO2 < 70–80 mmHg
Stage 2⁉️
Persistent hypoxemia → ↓ HCO3
Lowers pH toward normal
Removes alkalosis inhibition
Allows greater ventilatory response
Pulmonary Disease
Common in pneumonia, PE, interstitial fibrosis
Also pulmonary edema (though acidosis more common)
Hyperventilation may be due to hypoxemia
Often not corrected by oxygen
Other contributors
Mechanoreceptors in airways, lungs, chest wall
Signals via vagus nerve
Juxtacapillary receptors (interstitium)
Irritant receptors (epithelium)
Activated by inflammation or inhaled irritants
(asthma, pneumonia)
These contribute to dyspnea even without hypoxia
Direct Stimulation of Medullary Respiratory Center
Cortical input (psychogenic hyperventilation)
Retained amines in hepatic failure (not prostaglandins⁉️)
Bacterial toxins (gram-negative sepsis)
Salicylates
Progesterone (pregnancy, luteal phase)
Persistent acid CSF after rapid correction of metabolic acidosis
NaHCO3 raises extracellular pH
Peripheral chemoreceptors reduce ventilation → ↑ pCO2
CO2 crosses BBB rapidly, HCO3 does not
Brain senses ↑ pCO2 → ↓ CSF pH
Paradoxical prolongation of hyperventilation
Neurologic disorders
Pontine tumors → local acidosis → ↓ CSF pH → ↑ ventilation
Hypocapnia in acute cerebral accidents
Mechanical Ventilation
Overventilation can cause respiratory alkalosis
Correct by
Increasing dead space (no explanation given 🤷🏻♂️)
Decreasing tidal volume
Decreasing respiratory rate
SYMPTOMS
Due to increased CNS and peripheral nerve excitability
Lightheadedness
Altered consciousness
Paresthesias (extremities, circumoral)
Cramps
Carpopedal spasm
Syncope
Cardiac
Supraventricular and ventricular arrhythmias
Mechanisms
Impaired cerebral function
Increased membrane excitability
↓ cerebral blood flow
35–40% reduction if pCO2 drops by 20 mmHg
Psychogenic hyperventilation symptoms
Dyspnea
Headache
Chest pain
Symptoms more prominent in acute disease (rapid pH change)
Electrolytes
↓ phosphate (as low as 0.5–1.5 mg/dL)
Due to intracellular shift
Increased glycolysis → ↑ phosphorylated compounds
DIAGNOSIS
Tachypnea
But could be acidosis or alkalosis
Consider sepsis
Compensation equations can be ambiguous
Example: 7.48 / 20 / XX / 16
Could be chronic respiratory alkalosis
Or acute respiratory alkalosis + metabolic acidosis 😖
Case 21-1
5-year-old with AMS, playing with aspirin
TREATMENT
Usually not necessary
Do NOT give
Respiratory depressants
HCl
Paper bag rebreathing
↑ inspired CO2
Can correct acute respiratory alkalosis
If chronic → may leave patient with metabolic acidosis
Can treat with NaHCO3
“Give a mouse a cookie” 😉