Chapter Two: Renal Circulation and Glomerular Filtration Rate, part 1
Back by popular demand…all two of you…the second chapter of The Clinical Physiology of Acid Base and Electrolyte Disorders.

Chapter Outline
- Renal Circulation and GFR
- RBF is 20% of cardiac output
- In terms of mL per 100 g organ weight it is 4x the liver and exercising muscle and 8x coronary blood flow!
- After the glomeruli the efferent arteriole have two fates
- Peritubular capillaries in the cortex
- Peritubular capillaries are not necessarily associated with their parent glomeruli. Weird.
- Vasa recta from juxtamedullary glomeruli in the medulla
Joel Says: This seems wrong. Solute balance can be maintained down to a very low GFR. The R^2 here would be very low. Prove me wrong.
- States that GFR is an important determinant of solute and water excretion.
- Glomerular anatomy and function
- Structure
Four editions of the Bud Bible up top and a copy of Bud Light on the bottom.
- Glomerulus is a tuft of capillaries
- Enclosed in a capsule of epithelial cells, called Bowman’s capsule
- The epithelial cells of Bowman’s capsule are continuous with the epithelial cells of the proximal tubule

Looking at scanning EMs of the glomerulus is one of life’s simple pleasures—Josh.
Josh says: Look at the review in Nature Reviews Nephrology from Rachel Lennon’s group
- Filtration barrier
- Epithelial cell (podocyte)
- Epithelial cells adhere to the basement membrane via foot processes and the foot processes have slit diaphragms
- Basement membrane
New Super-resolution structure of the GBM: https://elifesciences.org/articles/01149 Hi res microscopy is really hi-res. Technique is call ed STORM.
Melanie talks about conduits through the glomeruli. Here is a cool review:
Why until just now? Undiscovered uniqueness of the human glomerulus! by L. Gabriel Navar, Owen Richfield
Am J Physiol Renal Physiol. 2018 Nov 1; 315(5): F1345–F1346. Published online 2018 Aug 15. doi: 10.1152/ajprenal.00369.2018 PMCID: PMC6293291
- Produced by both the endothelial cells and podocytes
- Formed from type IV collagen
- Abnormalities of type 4 collagen cause Alport
- The gene coding for the alpha 5 chain is the culprit
- COL4A5
- Abnormal Alpha 3 and 4 chains can also cause hereditary nephritis
- Has other substances
- Laminin
- Nidogen
- Heparin sulfate proteoglycans
- Provides the negative charge
- Enthothelial cell (fenestrated)
- Protein excretion
- Glomerular function: allow filtration of small solutes (Na and urea) while preventing filtration of larger molecules
- Insulin MW 5,200 is freely filtered (upper range of freely filtered)
- Preventing loss of protein prevents
- Negative nitrogen balance
- Development of hypoalbuminemia
- Infection from loss of immunoglobulin
- Size and charge selectivity of the GBM
- pores are between cords of type 4 collagen
- The epithelial cells and slit diaphragms matter
- Macromolecules that pass through GBM can accumulate underneath the epithelial layer
- Isolated GBM in invitro studies is much more permeable to than intact glomerulus
- There is increased protein filtration in areas where the epithelial cells have detached from the GBM

Josh really likes this figure from another Nature Reviews Nephrology paper. This one by Moeller and Chia-Gil.
- Mutations in nephrin, localized to the slit diaphragm causes congenital nephrotic syndrome
- Charge selectivity is important
- Neutral and cationic particle are more likely to be filtered
- Albumin (negative charge) is filtered 5% as well as same size neutral dextrans
- In glomerular disease, while there is increased filtration of proteins there is decreased filtration of small solutes due to loss of glomerular surface area
JC says: Take a look at this research on the serving coefficient in glomerular disease. Some surprising results.
Glomerular dysfunction in nephrotic humans with minimal changes or focal glomerulosclerosis
- Why do people in remission have what appears to be spilling more high molecular radius particles than normal and why do patients with active MCD have lower clearance across all molecular diameters?
- Other glomerular functions
Josh says: Take a look at this interesting paper by Butt et al
A molecular mechanism explaining albuminuria in kidney disease
- Synthetic
- Epithelial cells produce GBM
- Phagocytic
- Remove circulating macromolecules that pass through GBM and get trapped in subepithelial space
Josh says: The sFLT1 (soluble VEGF receptor) relationship to preeclampsia is just so cool. And here’s the paper:
And in the NEJM: VEGF Inhibition and Renal Thrombotic Microangiopathy
- Endocrine
- Enthothelial cells regulate vascular tone by releasing
- Prostacyclin
- Endothelin
- Nitric oxide
JC says: Do yourself a favor and spend some time learning about extraglomerular mesangial cells with Stuart Shankland
Joel adds, if you ever get a chance to party with Dr. Shankland, don’t skip out.
- Mesangial cells, two types
- Intrinsic Mesangial cell
- Microfilaments similar to smooth muscle
- Responds to Ang2
- Regulates glomerular hemodynamics
- Can release cytokines
- Can respond to cytokines by proliferation
- Circulating macrophages and monocytes
- Phagocytic function
- Clear molecules that get through the endothelial wall but cant get through the GBM
Josh says, “Topf, get it right. Its Ree-nin not renin. Classic letter to JAMA.

- Renin-Angiotensin System
- Afferent arteriole contain specialized cells called juxtaglomerular cells
- Produce prorenin which cleaved into renin
- Stimuli for renin release
- Hypotension
- Volume depletion
- Increased sympathetic activity
- Renin catalyze the production of ang1 from angiotensinogen
- Ang1 is catalyze to Ang2 by ACE located in the
- Lung
- Endothelial cells
- Glomeruli itself
- Discussion of local renin and Aniotensinogen
- Explains why ACEi are useful even with low systemic renin levels and Ang2
- Actions of Ang2
- Sodium and water retention
- By direct Na reabsorption in the early PT (and in the proximal tubule, water is permeable to the epithelium so every sodium reabsobed, brings a water molecule along for the osmotic ride.
- Stimulates the Na-H antiporter
- 40-50% of Na reabsorption in the S1 segment of the PT is due to Ang2
- By stimulation of aldosterone
- Ang2 that stimulates Aldo comes from the kidney and from the adrenal gland itself
- Vasoconstriction
Josh talks angiotensin:
Tenses the angios--love this Melanie!
1961 paper from del Greco (who's endowed chair Dan Batlle has now) trying AT2 in "hopeless" patients and dialysis patients:
https://jamanetwork.com/journals/jama/article-abstract/332265
Great EM-crit/pulmcrit discussion here:
https://emcrit.org/emcrit/deeper-vasopressors-athos-3/
and caveats here:
https://emcrit.org/pulmcrit/angiotensin-ii/
- Arteriolar vasoconstriction
- Ang2 important for raising BP in RAS
- Ang2 important in maintaining BP with volume depletion or in CHF, liver disease
- Giving ACEi to cirrhosis can cause BP to dump 25 points
- Regulation of GFR
- Affects constriction at afferent arteriole and efferent arteriole
- Mediated via thromboxane
JC talks about the ATHOS trial and how there is a signal for improved outcomes especially in patients requiring renal replacement therapy.
- Afferent arteriole starts bigger so reductions have less of an effect than constriction does on the narrower efferent arteriole.
- This results in a fall of RBF due to increased resistance but maintaining GFR by increasing inrtaglomerular pressure.
- Also stimulates prostaglandins which are vasodilator, modulating this affect
Joel says: You haven’t heard of the Trolly Problem? Oh you need to take 5 minutes and read this.
- It can stimulate contraction of the mesangium reducing surface area of the glom reducing filtration.
- It sensitizes the afferent arteriole to TG feedback so it can reduce glomerular flow in response to increased chloride detection in the TLoH.
- Control of renin secretion
Ever wanted to know about intrarenal renin concentrations? Yeah, me neither. But JC’s got you covered:
Endogenous angiotensin concentrations in specific intrarenal fluid compartments of the rat.
- Primarily sodium intake, increased intake results in less renin
- Mediated by baroreceptors
- Baroreceptors in afferent vessel wall
- Cardiac and arterial baroreceptors which activate the sympathetic nervous system and catecholamines which then stimulates renin
Roger says: Do your self a favor and read about Yanomamo Indians
Blood pressure and electrolyte excretion in the Yanomamo Indians, an isolated population
- Cells of the macula densa in the early distal tubule which detect decreased chloride delivery
- This allows loop diuretics to be particularly effective at increasing renin as they block chloride resorption
- Suppression of renin in response to chloride is mediated by adenosine
- Stimulation of renin in response to decreased chloride is mediated by PGE
- The PGE cause local vasodilation so the kidney maintained a rich blood flow while using renin and Ang2 to cause systemic vasoconstriction
Anna’s notes for the deep dive in glomerular barrier
Our understanding is based on technology available at the time. Even in 1920s, there was thought that tubular reuptake of protein may be important, but studies never demonstrated this til 2007 and even then are debated.

2007 Russo, et al (and BM at IU!) showed that The normal kidney filters nephrotic levels of albumin and that failure of retrieval by proximal tubule cells is what separates proteinuria from nonproteinuria. This was countered by a study in 2009 demonstrating much lower GSC and suggesting that the high GSC in the 2007 could be the result of nonphysiologic states.
Check out this 2008 debate in JASN regarding the validity of the charge model and “normal” albumin in the glomerular filtrate. Hotly debated with too many studies to cite.
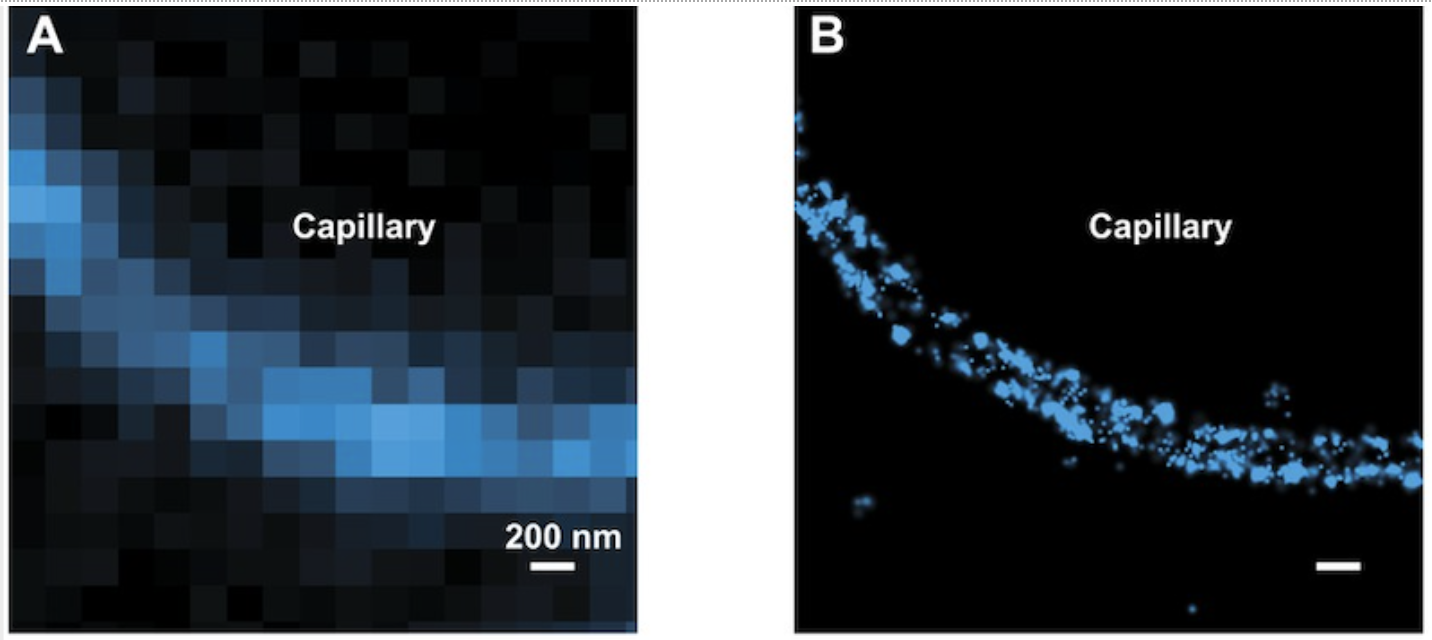
2017: Lawrence et al publish their findings that the GBM and podocyte processes are sufficient and the slit diaphragm likely does not exist. They used labeled proteins and confocal microscopy to determine migration of particles through the enodthelium and GBM. They also injected NaSCN oligoclusters from the size of albumin (66kDa)up to the size of IgG dimers (300 kDa) into mice, then fixed. The size-sensitive permeation into the lamina densa of the GBM and the podocyte glycocalyx of albumin and uptake of any “escaping” albumin by the proximal tubule was also observed. This countered the common prior conception that the slit diaphragms pores are the site of albumin “capture.”



For your reading pleasure the review of Clinical Physiology of Acid-Base and Electrolyte Disorders Fourth Edition in Annals of Internal Medicine